Acne was first identified as a disease by dermatologists in the nineteenth century.
Epidemiology of Acne Vulgaris
According to the Global Burden of Disease (GDB) study, acne vulgaris affects 85% of young adults aged 12–25 years.
Pimple is the most commonly treated dermatologist condition.
A lifetime prevalence of more than 90% means almost 100% of people will experience acne in their lifetime.
Acne is a universal condition in the younger population.
Moderate to severe acne affects around 20% of the young population, and its severity depends on pubertal maturity.
It is most common at a young age because of earlier puberty. Black individuals are more susceptible to post-inflammatory hyperpigmentation.
Most acne persists into the 20s to 30s in around 64% and 43% of individuals, respectively.
Heritability of acne is almost 80% in first-degree relatives, and for those who have a positive family history, acne comes earlier and is more severe for them.
Socio-economic burden
Acne can affect more than just your skin; it can affect your emotional health, cause decreased self-esteem, and cause psychological distress.
Acne costs 3 billion dollars per year in the USA for treatment and loss of productivity.
Acne vulgaris was graded by Indian authors using a simple grading system, which classifies acne vulgaris into four grades as follows:
Grade 1: Comedones, occasional papules.
Grade 2: Papules, comedones, and a and a few pustules.
Grade 3: Predominant pustules, nodules, and abscesses.
Grade 4: Mainly cysts, abscesses, and widespread scarring.
Clinical classification of acne vulgaris
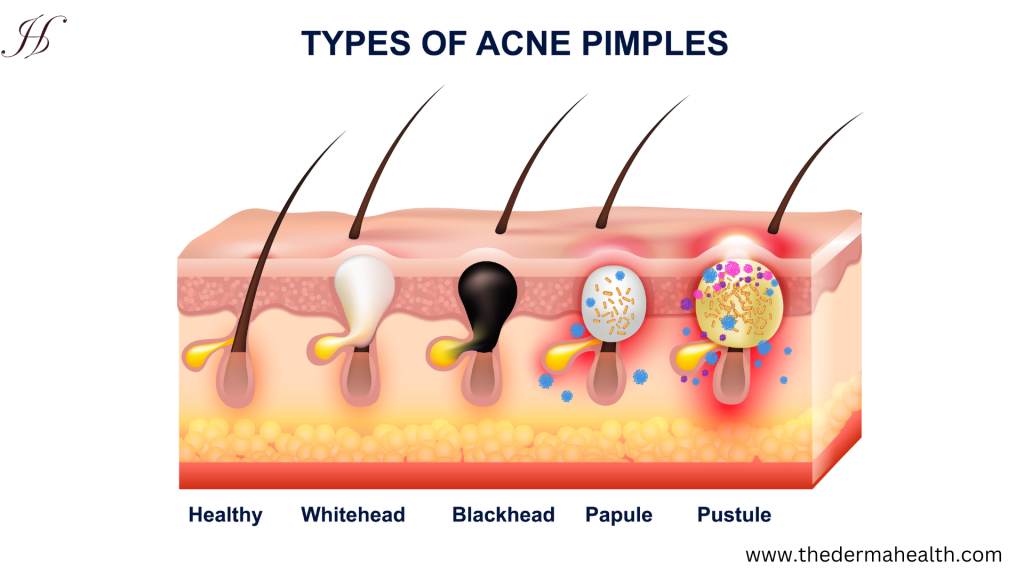
Types of acne
Comedones
Papules and pustules
Nodules and cysts
Mild (Non- inflammatory)
Comedones are the main lesions less than 20.
Small and few in papules and/or pustules
No nodules or cysts
Moderate (Inflammatory)
10–40 comedones
10–40 papules and/or pustules
Nodules 0–10 But no cysts
Severe
40–100 comedones
More than 40 papules and/or pustules
Nodulocystic acne (Nodules > 10; many cysts)
Common sites of acne
Acne lesions can be present in various parts of the body, primarily in the face, chest, neck, shoulder, and back, because these parts of the body have more sebaceous glands (oil glands), and hair follicles are connected to sebaceous glands.
Causes of acne vulgaris
Excess oil (sebum) production: sebaceous glands produce sebum, an oily substance that lubricates the skin. Overproduction of sebum can clog pores, leading to acne formation.
Clogged pores: blackheads and whiteheads develop when dead skin cells, bacteria, and extra oil build up in hair follicles and form plugs.
Propionibacterium acnes (Cutibacterium acnes), or P. acnes, is a type of bacteria that is typically found on the skin. When pores become clogged, P. acnes multiplies, causing inflammation and the development of inflammatory acne lesions.
Hormonal fluctuations: changes in hormonal levels like high androgen (testosterone) hormone, especially during puberty, menstruation, pregnancy, and menopause, birth control pills, and stress.
Genetics, or positive family history, runs within the family. Studies show both parents who have acne children have more chances to develop severe acne at an early age.
Gender: women have a higher chance of developing adult acne during periods, pregnancy, and polycystic ovary syndrome.
Some factors may trigger acne:
Excessively touching, resting on, or rubbing the skin.
People of all ages can get acne, but it’s most common in teenagers.
Hormonal changes are common during puberty or pregnancy. Androgens are hormones that increase in boys and girls during puberty and cause the sebaceous glands to enlarge and make more sebum. Hormone changes during midlife, particularly in women, can lead to breakouts too.
Family history and genetics play a role in acne. If both of your parents had acne, you’re likely to develop it too.
Greasey or oily substances may cause you to develop acne when your skin comes into contact with oily lotions and creams.
Friction or pressure on your skin can be caused by items such as telephones, cellphones, helmets, tight collars, and backpacks.
Examples of certain medications include drugs containing corticosteroids, testosterone, or lithium.
Studies indicate that consuming certain foods—including carbohydrate-rich foods such as bread, bagels, and chips—may worsen acne.
Stress doesn’t cause acne, but if you already have acne, stress may make it worse.
Pathophysiology of acne vulgaris
The skin’s sebaceous gland and hair follicles are part of the pilosebaceous unit, and acne vulgaris is a disease that is typically classified as either inflammatory or noninflammatory.
The etiology of acne, which involves androgenic hormones like testosterone, typically shows up during puberty. And after puberty, it usually goes away, but not always.
Two groups of etiological factors that can contribute to developing acne are:
Genetics: a person with oily skin or a positive family history has a higher chance of developing acne.
Environmental: heat and humidity, pressure, and friction like helmets, hands, etc. Diet—high-glycemic-index foods like processed food, sugar-containing beverages, first food, bakery items, potatoes, etc.
Hormone:
Excess androgen is one of the initial products that does increase keratin production, also called epithelial/keratin hyperproliferation. Keratin is a hair and skin protein that is found in the sebaceous gland or hair follicle of the face and upper trunk.
This hyperkeratinization can lead to the formation of the keratin plug. When this plug blocks the sebaceous gland opening, it can trap sebum or fatty acid within the hair follicle or sebaceous gland.
The trapping of sebum by the keratin plug will lead to non-inflammatory acne lesions called white and black heads.
Another reason it occurs after puberty is that not only does excess androgen increase keratin production, but it also causes an increase in the sebum and the presence of more proinflammatory lipids as opposed to non-inflammatory or anti-inflammatory lipids.
This process will continue if bacteria colonize the trapped sebum.
This bacteria colonized this trapped sebum to cause inflammatory acne known as papules, pustules, nodules, and cysts.
Furthermore, this inflammatory acne has a tendency to burst, which allows its contents—including more bacteria—to be released into the dermis, or top layer of the skin. This may result in more pimples and prolong the acne growth cycle.
Presentation of Acne vulgaris
Acne signs vary depending on the severity of your condition:
Whiteheads (closed, plugged pores)
Blackheads (open-plugged pores)
Papules (small, red, tender bumps)
Pustules (which are papules with pus at their tips)
Nodules (large, solid, painful lumps under the skin)
Cystic lesions (painful, pus-filled lumps under the skin)
Management of acne vulgaris
Diagnosis of acne:
The diagnosis of acne is mostly based on a clinical or visual examination of the lesions.
To screen for infection, a bacterial culture may occasionally be done.
History of acne patients:
Current age and onset of acne.
Medical and drug histories.
Positive family history.
In women, a history of periods must be taken, together with the frequency and association with acne outbreaks.
Treatments:
Self-care is the key to getting rid of acne.
Cleanse skin gently with a mild, nondrying cleanser.
Look for water-based or non-comedogenic formulas for cosmetic and skin creams.
Remove all dirt or make-up. Wash twice a day, including after exercise.
Avoid scrubbing or repeated skin washing.
Shampoo your hair frequently, especially if it is oily.
comb or pull your hair back to keep the hair out of your face.
Topical creams or gels applied to the skin may be prescribed:
Derivatives of vitamin A, such as retinoic acid cream or gel (tretinoin, tazarotene).
Prescription formulas of benzoyl peroxide, sulfur, resorcinol, or salicylic acid.
Topical azelaic acid.
Topical corticosteroids (hydrocortisone) reduce inflammation in cases of inflammatory acne. Always use lower potencies first.
Oral medications—antibiotics (tetracycline, doxycycline), hormonal medications (spironolactone), and isotretinoin—are helpful for severe or persistent acne. Minocycline (1st choice for acne), doxycycline (2nd choice for acne), and sarecycline only give non-nodular moderate-severe acne.
Side effects include photosensitivity, permanent tooth discoloration.
Women taking isotretinoin must not be pregnant and do regular blood tests.
Pregnant women should NOT take isotretinoin because it causes severe birth defects.
Hormone Spironolactone (an aldosterone receptor antagonist) gives an anti-androgen effect; it is not FDA-approved but is used in women. Oral contraceptives (estrogens) are good for the menstruation cycle.
Lifestyle modifications—a regular skincare routine, good hygiene, maintaining a healthy diet, managing stress, and avoiding picking or squeezing pimples—help prevent and cure acne.
Other treatment options:
A small randomized control trial (RCT) showed that low-glycaemic index (GI) diets can lower acne severity, but this remains unproven.
Initially, our primary goal was to reduce or stop four primary mediators of acne pathophysiology:
Increase androgen levels to reduce hyperkeratinization and abnormal sebum.
Hyperkeratinization is reduced by:
Salicylic acid reduces hyper keratinization by interfering with cell-cell adhesion; avoid it if the patient is under aspirin.
Benzoyl Peroxide (BPO) reduces hyper keratinization by cell-cell adhesion, reduces bacteria colonization by releasing free radicals, and decreases irritating fatty acids. Photosensitivity: do go out with it; do dry skin.
Topical retinoids decrease hyperkeratinization by decreasing adhesion and increasing turnover. Avoid pregnancy, limit sun exposure, and avoid salicylic acid.
Isotretinoin, or oral tretrion, reduces hyper keratinization by decreasing adhesion and increasing turnover. Decrease sebum production. Oral capsule, not in pregnancy (do severe teratogenicity), dry skin, lips, eyes. Increased TG, back pain, arthralgia, osteoporosis, and ocular dysfunction. Give for a 15–20-week course.
Abnormal sebum production is reduced by antiandrogens, isotretinoin, topical and oral antibiotics, corticosteroids, and estrogen.
Bacterial colonization and proliferation are caused by benzoyl peroxide, topical and oral antibiotics, and isotretinoin.
General or inflammatory response: intralesional corticosteroids, oral corticosteroids, topical or oral antibiotics.
Prognosis (Outlook)
Most of the time, acne goes away after the teenage years, but it may last into middle age. The condition often responds well to treatment, but responses may take 6 to 8 weeks, and acne may flare up from time to time.
Scarring may occur if severe acne is not treated. Some people become very depressed if acne is not treated.
Does and Don’t
Not to aggressively squeeze, scratch, pick, or rub the pimples; this can lead to infection and scarring.
Avoid tight headbands, baseball caps, and other hats.
Avoid touching your face with your hands or fingers.
Avoid greasy cosmetics or creams.
Do not leave makeup or cream on overnight.
Remove all dirt or make-up, and wash twice a day.
Avoid scrubbing or repeated skin washing.
Shampoo your hair daily if it is oily.
Comb or pull your back to keep hair out of your face.
A small amount of sun exposure may improve acne slightly.
When seeking medical help
Self-care and over-the-counter medicine do not help after several months.
Your acne is very bad, with lots of redness around the pimples or cysts.
Acne is getting worse.
Develop scars as your acne clears up.
It causes emotional stress.
Complications of acne vulgaris
People with darker skin types are more likely than people with lighter skin to experience these acne complications.
Scars are the most common complication after acne healing.
Skin tones change: after acne has cleared, the affected skin may be darker (hyperpigmented) or lighter (hypopigmented) than before the condition occurred.
Psychological effects: it has significant psychological effects, including low self-esteem, depression, anxiety, and social withdrawal.
Infection: picking or squeezing acne lesions can introduce bacteria into the skin, causing infectious acne.
Keloids: in some cases, especially with genetic predisposition, severe acne lesions can form keloids.
Dermatological complications, such as folliculitis (inflammation of hair follicles), rosacea (chronic facial redness), and seborrheic dermatitis (patches on the scalp and face).
Myths about acne vulgaris
Chocolate and greasy foods: eating chocolate or greasy food has little to no effect on acne.
Hygiene: acne isn’t caused by dirty skin. In fact, scrubbing the skin too hard or cleansing with harsh soaps or chemicals irritates the skin and can make acne worse.
Cosmetics: cosmetics don’t necessarily worsen acne, especially if you use oil-free makeup that doesn’t clog pores (non-comedogenic) and remove makeup regularly. Non-oily cosmetics don’t interfere with the effectiveness of acne drugs.
Squeezing blackheads, whiteheads, and spots is the best way to get rid of acne.
Sexual activity can influence acne.
Acne is infectious and can be passed on to other people.
Acne is removed by toothpaste.
Sun exposure cleans acne; it temporarily dries out pimples, but in the long run, it causes skin dehydration and inflammation.
Natural sunlight and poor hygiene are not associated with acne.
Frequently Asked Questions (FAQ)
How can I prevent acne?
Maintaining good skin care habits, such as washing your face regularly with a gentle cleanser, avoiding touching your face with dirty hands, and using non-comedogenic (non-pore-clogging) skincare products, can help prevent acne.
Does diet affect acne?
Although there is a lack of evidence about the relationship between diet and acne, certain foods that are high in sugar, dairy, and refined carbs may make acne worse in certain people. Healthy skin may result from eating a balanced diet full of nutritious grains, fruits, vegetables, and lean meats.
What are some treatment options for acne?
Acne treatment options vary according to the severity of the condition. Mild acne can be treated with over-the-counter topical treatments that include chemicals like retinoids, salicylic acid, or benzoyl peroxide. Prescription drugs such as oral antibiotics, hormone treatment, or isotretinoin may be required in more severe cases. Dermatologists may also recommend on-site treatments like chemical peels, laser therapy, or so on.
Should I pop my pimples?
It’s generally not recommended to pop pimples, as it can worsen inflammation, lead to scarring, and spread bacteria, causing more breakouts.
How long does it take for acne to clear up?
The time it takes for acne to clear up varies from person to person and depends on factors like the severity of the acne, the treatment used, and individual skin characteristics. Mild acne may clear up in a few weeks with proper treatment, while more severe cases may take several months to improve.
Can stress cause acne?
No, stress does not cause acne, but stress can exacerbate acne in some individuals by triggering hormonal changes that increase oil production in the skin. Managing stress through techniques like exercise, meditation, and relaxation can help improve acne symptoms.
Can I wear makeup if I have acne?
Yes, if you have acne, you can still apply makeup, but to avoid further clogging of your pores, make sure the items you choose are oil-free and non-comedogenic. To avoid buildup and potential breakouts, make sure to remove any makeup completely before going to bed.
When should I see a dermatologist for acne?
It’s recommended to visit a dermatologist for individualized treatment recommendations if over-the-counter medicines aren’t controlling your acne or if you have severe or persistent acne that’s impacting your quality of life or leaving scars.
Does acne damage skin?
Scarring is the most common acne problem if the acne extends deep into the skin. Any type of acne can cause permanent harm to the skin.
At what age do most people get acne?
An estimated 85% of teens get acne; girls between the ages of 14 and 17 and boys between the ages of 16 and 19 are more likely to have acne. When a person reaches their mid-20s, acne frequently goes away. Acne can occasionally persist until maturity.
Is acne difficult to cure?
Severe acne can be difficult to treat, but most acne is possible to clean. It is recommended to see a dermatologist for acne treatment.
If acne goes deeper into the skin and is damaged, it makes a permanent scar, called pick marks or acne scars. It is a concave shape that looks like a hole in the skin.
Are acne scars genetic?
Yes, DNA can play a role in your scars because your genes play a significant role in how your skin heals, and collagen production and the depth of acne also play a role in acne scars.
Is a lack of sleep a cause of acne?
Yes, due to a lack of sleep, the body could make excess cortisol hormone, which can cause more acne. So good sleep is key to staying healthy, both for the skin and the body.
Does digestion cause acne?
Prolonged digestion increases the opportunity for gut microbes and their metabolites to enter the circulation. From there, they can affect cell activity and cause inflammation, both of which may result in acne and negatively impact your health.
Can viruses and bacteria cause acne?
Yes, Cutibacterium acne can cause acne, but it is not contagious. Disruption of normal skin flora can cause overgrowth of Cutibacrerium acne, which leads to the development of acne.
How do I apply acne cream?
The ideal way to apply the cream directly on top of blemishes and spots is to leave it overnight for the best result.









Leave a Reply